This is the second of three blogs discussing phantom limb pain. Please look in the archive for the first which discussed prevalence and characteristics of the problem.
While phantom limb pain has been reported for hundreds – if not thousands of years, its causes have been unknown until recently. As recently as the American civil war, everybody “knew” that people could still feel their amputated limbs. Thus, if a person reported burning sensations from the phantom, it was because the amputated limb had been burned. The same logic applied to crawling feelings (worms in buried limbs), and biting feelings (fish eating limbs thrown into lakes). More recently, clinicians realized that people couldn’t actually feel what was happening to their amputated limbs. Sadly, the general conclusion was that the problem must stem from psychological problems such as the “pain” of “grieving” for the lost limb. Surgeons felt that there must be something wrong with the remainder of the limb – even if they didn’t know what – so frequently cut off more of the stump to solve the problem. Without actual evidence of underlying physiological and anatomical causes for phantom pain, there was no way to develop mechanism based interventions. Thus clinicians eventually wound up trying over 63 unrelated treatments – ranging from benign massages through horrible neurosurgical procedures – on many thousands of amputees. No actual follow-up studies of their effectiveness were performed so clinicians didn’t realize until recently that nearly all were useless. Many of these unsubstantiated interventions are still being used today. More on this in the next blog on treatments.
For now, it is crucial to know that the actual physiological mechanisms causing burning and cramping descriptions of phantom pain have been identified. The remainder of this blog discusses the strength of the evidence supporting this assertion. Knowledge of mechanisms has led to development of effective treatments for these descriptions of phantom pain which will be discussed in the next blog entry. The mechanisms underlying shocking phantom pain have not been clearly identified and treatments for this description are still ineffective.
Relationships Between Phantom Limb Pain And Muscle Tension
(Much of the information in this section is adapted from the book “Phantom Pain” by Richard Sherman).
Chronholm (1951) quotes Amyot (1929), Livingston (1943) and others as having noted increased muscle tension and spasms in the stumps of amputees. He found that 51 of 99 amputees questioned about stump muscular activity reported spontaneous hyperactivity.
Onset and intensity of cramping and squeezing descriptions of phantom pain are related to muscle tension in the residual limb. A variety of studies have demonstrated that intensity of cramping phantom pain and amount of muscle tension in the residual limb change together both from day to day (Sherman & Arena, 1992) and from moment to moment (Sherman et al., 1992).
Changes in surface electromyographic (EMG) representations of muscle tension in the residual limb precede changes in cramping and squeezing phantom pain by up to several seconds. This relationship does not hold for any other descriptions of phantom pain. The method for establishing this relationship is illustrated in Figure 1 and a typical recording from a bilateral amputee is illustrated in Figure 2. The critical point illustrated is that the amputee only shows changes in muscle tension in the painful residual limb. Surface EMG in the pain free residual limb does not change significantly. If the change in EMG was simply a reaction to the change in pain, the change in EMG would have followed, rather than preceded the change in pain and at least some change in muscle tension in the pain free limb should have been observed as would be expected from a generalized withdrawal reflex from pain.
Relationships between overall muscle tension in the residual limb and cramping phantom pain have also been shown to hold throughout the day in subjects’ normal environments (Sherman et al., 1993a). Figure 3 illustrates these relationships in two amputees with cramping phantom limb pain who wore an ambulatory recording device for two days. The device was capable of recording surface EMG from the residual limb and button press representations of pain intensity (Sherman et al. 1991). The relationship between cramping phantom pain and muscle tension in the residual limb is supported by the consistent success of treatments resulting in reduction of residual limb muscle tension for cramping phantom pain but not for other descriptions (Sherman 1976; Sherman et al., 1991; Sherman et al., 1992).
Numerous amputees report that cramping phantom pain decreases with any activity which tends to decrease muscle contraction levels in the residual limb and increases with activities increasing overall levels of contraction. Thus, such activities as phantom exercises which result in changes in muscle tension in the residual limb can result in temporary changes in intensity of phantom pain. Gessler (1981) reported that when the muscles of the residual limb of ten amputees with chronic cramping phantom pain were relaxed, the phantoms felt as though they were opening.
Figure 1. Methodology used to establish temporal relationships between change
in phantom pain intensity and change in surface EMG of the residual limb.
Both of the subject’s limbs are instrumented for recording surface electromyographic (EMG) representations of muscle tension (f). The signals are sent to a chart recorder (e) where they are displayed with line “i” showing the signal from the intact limb and line “h” showing the signal from the residual limb (stump). The subject presses button (d) when the intensity of phantom pain increases and lets go of the button when the intensity returns to its prior level. The button press signal is displayed on line “g”. The entire session is recorded both on paper and by a digital tape recorder (j).
Figure 2. Samples from a chart recording showing surface EMG from the residual limb and “button press” responses to changes in cramping phantom pain intensity made by a bilateral amputee.
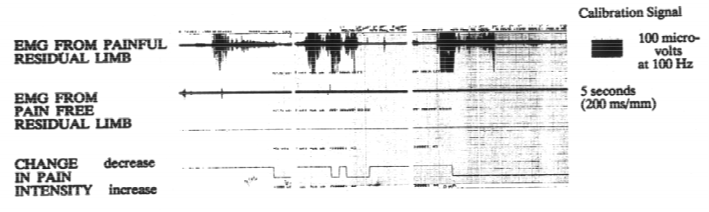
Figure 3. Relationships between cramping phantom pain and muscle tension in the residual limb recorded in subjects’ normal environments.

Burning – Tingling Phantom Limb Pain
(Much of the information in this section is adapted from the book “Phantom Pain” by Richard Sherman, Plenum, 1996).
Virtually all of the heat emanating from the limbs is caused by blood flowing just under the surface. Thus, measurements of limbs’ surface heat are highly correlated with near surface blood flow. The most common way to record heat emanating from the limb is with a videothermograph. These devices use infrared to measure heat and produce a colored “TV” like picture of heat patterns on the surface of the limb. Each color can be related to a specific temperature so the picture shows both the pattern of heat emanating from the limb as well as the actual temperatures of each area. Figure 4 illustrates a typical thermograph being used to take a heat picture of a hand.
Figure 4. Image produced by a thermograph
(Each color corresponds to a temperature.)

Reduced near surface blood flow to a limb has been implicated as a predictive physiological correlate (first cousin to a cause) in many pain conditions including causalgia and reflex sympathetic dystrophy (Karstetter et al., 1991). Return of blood flow to normal patterns through any intervention, including time alone, usually results in either the complete cessation or significant decrease of the pain (Sherman et al., 1991). If phantom limb pain is a referred pain syndrome, anything effecting the nerve endings in the residual limb is likely to affect phantom pain as well. A number of excellent studies have demonstrated that (a) the ends of the nerves which used to serve the amputated limb are still sensitive to stimuli, (b) cooling the nerve ends causes increased firing rates, and (c) reducing blood flow to the extremity results in it becoming cooler (Campbell, 1987; Janig, 1987; Harber, 1955; Koschorke et al., 1987; Matzner & Devore, 1987; Sherman & Arena, 1992).
Chronholm (1951) quotes Pitres (1897) as having stated that the perceived temperature of the phantom is related to the temperature of the stump. Measurements of skin temperature in amputees have been made since at least 1952 (Studies relating… 1952). The study found that amputees’ residual limbs were cooler at the distal end than paired points on the opposite extremity and that the cooler areas did not warm up when attempts were made in increase cutaneous blood flow through such mechanisms as giving the subjects whiskey to drink.
Wahren (1990) reviewed the propensity of finger amputees to be very sensitive to the cold and for their pain to be aggravated by cold environments. They found that the residual areas of the fingers were cooler than corresponding areas on the intact hand and were more sensitive to pain in response to cooling. Kristen et al (1984) reported using videothermographic recordings of temperatures in the residual limbs of fifty amputees to detect phantom pain. They found that most amputees having phantom pain showed different patterns of temperature then those who did not.
Consistent, inverse relationships between intensity of phantom limb pain and temperature in the residual limb relative to that of the intact limb have been demonstrated for burning, throbbing, and tingling descriptions of phantom pain but not for any other descriptions (Sherman & Bruno, 1987). “It has also been established that (a) for these descriptors of phantom pain there is a day to day relationship between the relative amount of blood flow in the stump and pain intensity and that (b) there is an immediate change in pain when blood flow changes. However, this does not mean that the changes in blood flow cause the change in pain. It is possible that a change in pain intensity causes a physiological chain reaction which eventually causes a decrease in blood flow to the stump. This is improbable for several reasons. Although videothermographs normally record only near surface blood flow patterns, hands are thin enough so that thermographs can record blood flow patterns throughout the hand.
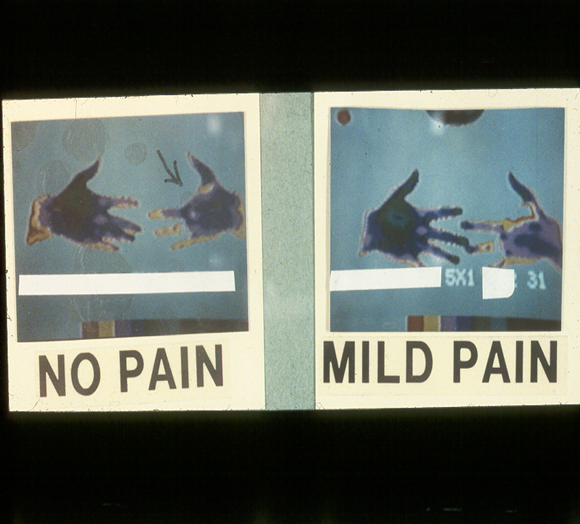
In four cases of burning or tingling phantom pain following a finger amputation, blood flow changed only in the area just proximal to the amputation site. The rest of the hand was essentially unchanged and there were no changes in the paired area of the intact hand. If blood flow was changing as a result of a reflex, we would have expected a bilateral change or, if unilateral, a change related to dermatomal distribution patterns in which an entire dermatome would have cooled off. This was not the case so we conclude that a reflex reaction is not likely. The subjects were taught to increase blood flow in the stump by using temperature feedback to relax, and thus dilate, the peripheral blood vessels. Increasing peripheral blood flow to the cool area of the stump resulted in a decrease in the pain intensity. If the decrease in blood flow was due to an increase in pain, blood flow would decrease for all descriptors of phantom pain, not just a consistent few” (Sherman & Arena, 1992). The relationship of burning phantom pain to blood flow in a bilateral amputee is illustrated in Figure 5.
This result and numerous thermograms like it form the key evidence that the decreased blood flow associated with burning phantom pain is not the subsequent result of a general sympathetic reaction because only the painful residual limb shows decreased blood flow ‑ the other residual limb maintains its temperature. Figure 6 illustrates the increase in burning phantom pain’s intensity with progressive decreases in surface blood flow in the residual limb. This tight relationship has been replicated numerous times (e.g. Sherman & Bruno, 1987) and indicates that there is more than a casual relationship between the two.
“The existence of a vascular related mechanism for burning phantom pain is also supported by the short term effectiveness of those invasive procedures, such as sympathetic blocks and sympathectomies, which increase blood flow to the limb and reduce the intensity of burning phantom and stump pain but not other descriptors (Sherman 1980 and Wall 1981). It is indirectly supported by the virtual ineffectiveness of every surgical procedure involving severing nerves either in the spinal cord or running between the amputation site and the spinal cord (Sherman &Sherman, 1985, Wall 1981). Beta blockers such as propranolol cause dilation of peripheral blood vessels and have been reported to be successful in ameliorating phantom pain at least in the short‑term (Marsland et al 1982)” (Sherman & Arena, 1992). Relationships between muscle tension and burning phantom limb pain (Sherman & Bruno, 1987) have been shown to be largely due to the change in near surface blood flow that accompanies increased muscle tension (Laughlin & Armstrong 1985; Richardson et al.1986).
Figure 5. Redrawn color videothermogram
of an above knee, bilateral amputee’s residual limbs
The right residual limb had a pain level of 0 while the left residual limb had burning phantom pain rated at an intensity of 2 on a scale of 0 ‑ 10. The size of the dots represents the temperatures in degrees Celsius recorded on the skin’s surface. Differences of less than one degree Celsius are within normal limits.
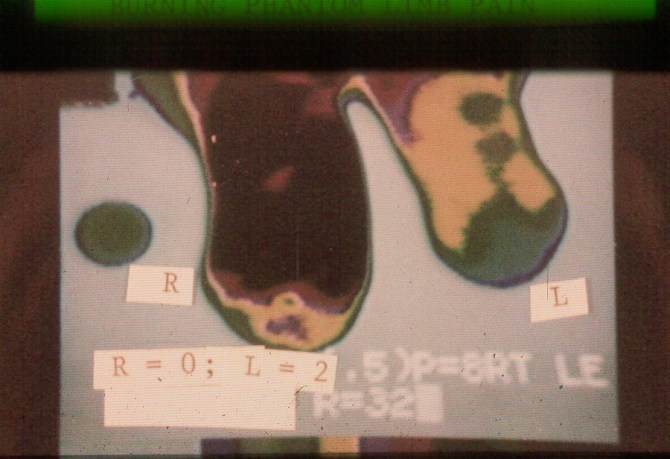
Figure 6.Redrawn color videothermograms
of an amputee missing the index finger on the left hand
Size of dots represents relative warmth at the skin’s surface with the largest dots showing the most warmth and blank areas being coolest. Blank areas are essentially the same temperature as the surrounding room. Burning phantom pain intensity is rated on a scale of 0 ‑ 10.
Supporting publications
Sherman R: Direct evidence of a link between burning phantom limb pain and stump blood circulation. Orthopedics 7:1319 ‑1320, 1984.
Sherman R, Bruno G: Concurrent variation of burning phantom limb and stump pain with near surface blood flow in the stump. Orthopedics, 10: 1395‑1402, 1987.
Sherman, R.: Phantom limb and stump pain. Chapter in (R. Portenoy, ed.) Neurologic Clinics of North America 7(2): 249‑264, W.B. Saunders Co., Publisher. 1989.
Sherman R, Griffin V, Evans C, Grana A: Temporal relationships between changes in phantom limb pain intensity and changes in surface electromyogram of the residual limb. Int. J. of Psychophysiology 13: 71 ‑ 77, 1992.
Sherman R, Arena J: Phantom Limb Pain: Mechanisms, incidence, and treatment. Critical Reviews in Physical and Rehabilitation Medicine 4: 1‑26, 1992.
Sherman R, Devor M, Jones C, Katz J, Marbach J: Phantom pain, New York, Plenum Press; 1996. (Book)
Flor H, Birbaumer N, Sherman R: Phantom limb pain. Pain: Clinical Updates 8: 1-4, 2000.
Sherman R: Pain Assessment and Intervention from a Psychophysiological Perspective. Association for Applied Psychophysiology, Wheat Ridge Colorado, 2012. (Book)