The lack of understanding the cause(s) of the phantom pain have resulted in a plethora of unsubstantiated treatments attempting to rectify theoretical problems. Due to the lack of follow-up studies, until recently, there was little realization that of the 63 or so unrelated treatments in use, none had more than a one percent effectiveness level according to huge surveys of amputees.
Results of treatments not based on correcting underlying problems:
Sherman et al (1997) have shown that of over 60 treatments reported in the literature for treatment of phantom limb pain, only those which address underlying mechanisms produce more than one percent, consistent success – when success is defined as significantly reduced pain for at least three months. The incredible variety of approaches aimed at every part of the body are illustrated in Figure 1. For example, sympathectomy and sympathetic blocks both help burning / tingling descriptions of phantom pain but not others because these interventions increase blood flow to the residual limb.
As may be recalled, amount of reduction of blood flow is highly correlated intensity of burning / tingling pain. Thus, increasing blood flow decreases the pain. Muscle relaxants tend to help cramping phantom pain but not others because any intervention which reduces muscle tension is likely to reduce the cramping sensations correlated with it. When the prosthetic is improperly fitted, it can cause restricted blood flow and crimp the nerves. Thus, correcting the problem with proper fitting can reduce phantom pain related to it. None of the other treatments including surgical revision of the residual limb, neurosurgery at any site, TENS, etc. had any consistent, lasting effect at all!
Figure 1. Treatments for phantom limb pain

Evidence that psychophysiological techniques are effective for preventing burning and cramping phantom limb pain:
It would be truly gratifying to be able to say that numerous controlled studies with long term follow-ups have clearly shown that burning and cramping phantom pain have been proven beyond any reasonable doubt to be amenable to applied psychophysiological interventions. Unfortunately, this is not the case. All of the author’s studies noted below as well as Harden et al’s (2005) time series analysis were successful open clinical studies with good follow-ups but no placebo controls.
1. Cramping phantom pain:
Nearly all of the amputees with cramping phantom limb pain who can learn to recognize the relationship between their pain and spikes in the surface EMG (muscle tension) of the residual limb and can learn to prevent the spikes from occurring, can prevent their phantom pain to the extent they can prevent the spikes. If the spikes continue, so will the cramping phantom pain. If the spikes can be voluntarily stopped once an episode of phantom pain begins, the episode can nearly always be almost entirely aborted. The author’s small studies showed that the vast majority of people can learn to control nearly all of their cramping phantom pain. Again, no learning equates to no control. Follow-ups of one to several years show that the results are sustained.
During treatment, the major muscles of the residual limb areinstrumented for SEMG biofeedback. As spasms are being looked for, the raw or nearly raw SEMG signal must be displayed. Any amount of averaging smoothes the signal so much that the brief spasms virtually disappear. Patients are taught to watch for spasms and to stop them. The vast majority of patients (well over 90% in the author’s experience) learn this skill within a few sessions and are able to prevent reoccurrence of cramping phantom pain for at least the several years for which patients are followed.
Some patients are very tense or don’t learn how to relax the limb so they have to be given progressive muscle relaxation training. This training does not result in reduction of the pain but does provide the skills needed to learn to stop the spasms when biofeedback is reinitiated after relaxation training is completed. About five percent of patients clearly show the spasms but don’t learn to control them. Some of these patients are helped by muscle relaxants.
2. Burning phantom pain:
The same premise holds true for burning as for cramping phantom pain. If patients can learn to increase blood flow to the residual limb, burning phantom pain will decrease to the extent that blood flow is normalized. The burning will remain away as long as blood flow remains normal. Unfortunately, about half of the author’s patients have not been able to learn to raise the blood flow in their residual limbs to a significant extent.
Burning – tingling descriptions are related to decreased blood flow so our interventions are centered on teaching patients to increase blood-flow to the residual limb. We do well with a combination of home practice of warming exercises such as autogenic suggestions, home use of thermometers as used for migraine patients, and temperature biofeedback in the clinic. We begin by training patients to control their hand temperature and then continue to teaching them to warm the residual limb. Surprisingly, even people who had their amputations due to vascular insufficiency seem to be able to learn to warm sufficiently to control the pain. Ten to fifteen percent of amputees do not learn to warm sufficiently to reduce their phantom pain significantly. These people are given trials of vasodilators as noted above. If they don’t work, we recommend sympathetic blocks.
Compilation of trials based on underlying mechanisms:
Among the author’s recent cases, EMG biofeedback was effective for thirteen of fourteen trials for cramping phantom pain. EMG biofeedback had minimal success with two and no success with ten of twelve trials for burning phantom pain. It had no success with eight trials of shocking phantom pain. Temperature biofeedback was ineffective for four trials of cramping phantom pain, was effective for six of seven trials with burning phantom pain, and had no success with three trials for shocking phantom pain. Nitroglycerine ointment (a topical vasodilator) was ineffective for one trial of cramping phantom pain and one of shocking phantom pain but successful for two trials of burning phantom pain. Trental (a blood viscosity enhancer) was ineffective for two trials of cramping phantom pain and one of shocking phantom pain. Nifedipine (a systemic vasodilator) was effective for three trials of burning phantom pain but ineffective for one trial of cramping and two trials of shocking phantom pain. Flexeril (a muscle relaxant) was effective for two trials of cramping phantom pain but ineffective for one of shocking phantom pain. Indocin (an anti‑inflammatory agent) was ineffective for two trials of cramping phantom pain. These medications have potential side effects and can not be used with many patients having a variety of medical problems. Thus, we prefer using self‑control oriented strategies to avoid these limitations.
A bit on how we do behavioral interventions for phantom limb pain
Instruments such as biofeedback devices help the therapist and patient recognize what is happening in the body and how well control strategies are working.
Biofeedback is an extremely important technique which every clinician of any background can incorporate into his or her practice.
Biofeedback is the process of using psychophysiological recording techniques to monitor one or more physiological parameters whose malfunction is causing the pain and showing the instantaneous levels of the parameters to the patient. The patient and therapist use the information to change the level at which the parameter is functioning from a pattern leading to pain to a pattern which avoids onset of the pain or stops the pain.
Biofeedback is an excellent tool for showing the therapist and patient what a physiological parameter (e.g. tension in the muscles of the residual limb or heat emanating from the limb) is doing. This process of recording and immediate display cannot be used alone for either assessment or treatment as it provides no integral interpretation of the display’s meaning. It has to be incorporated into some logical therapeutic process aimed at eliciting meaningful responses. Biofeedback is one tool among many in a professional’s armamentarium. It provides one bit of the information needed to make decisions and is only one element of the treatment process.
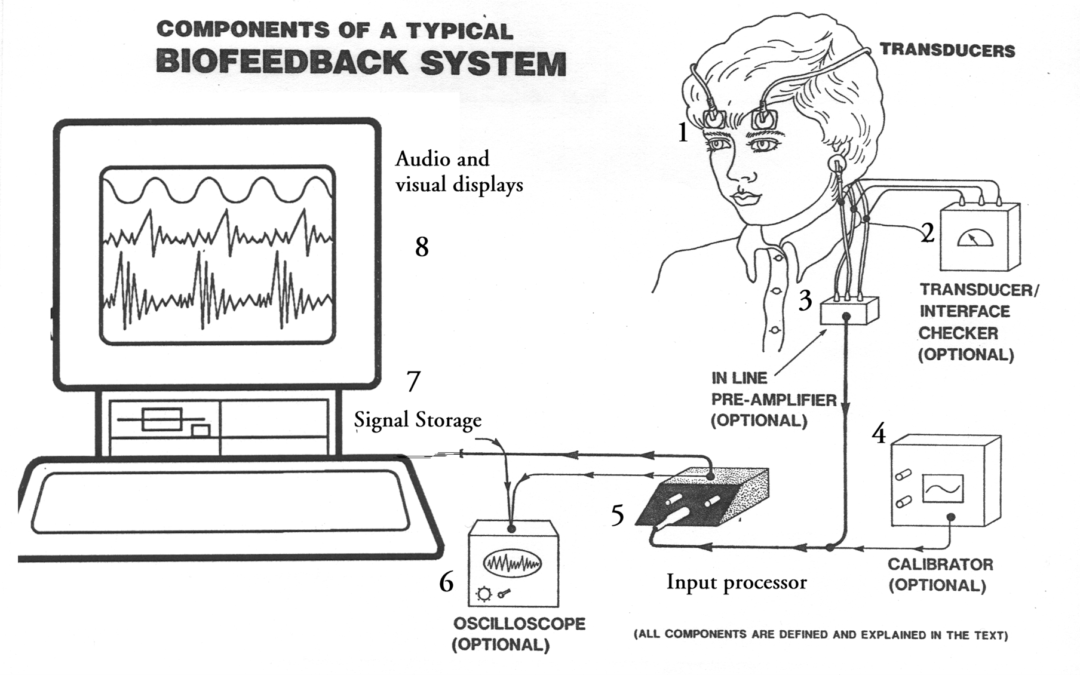
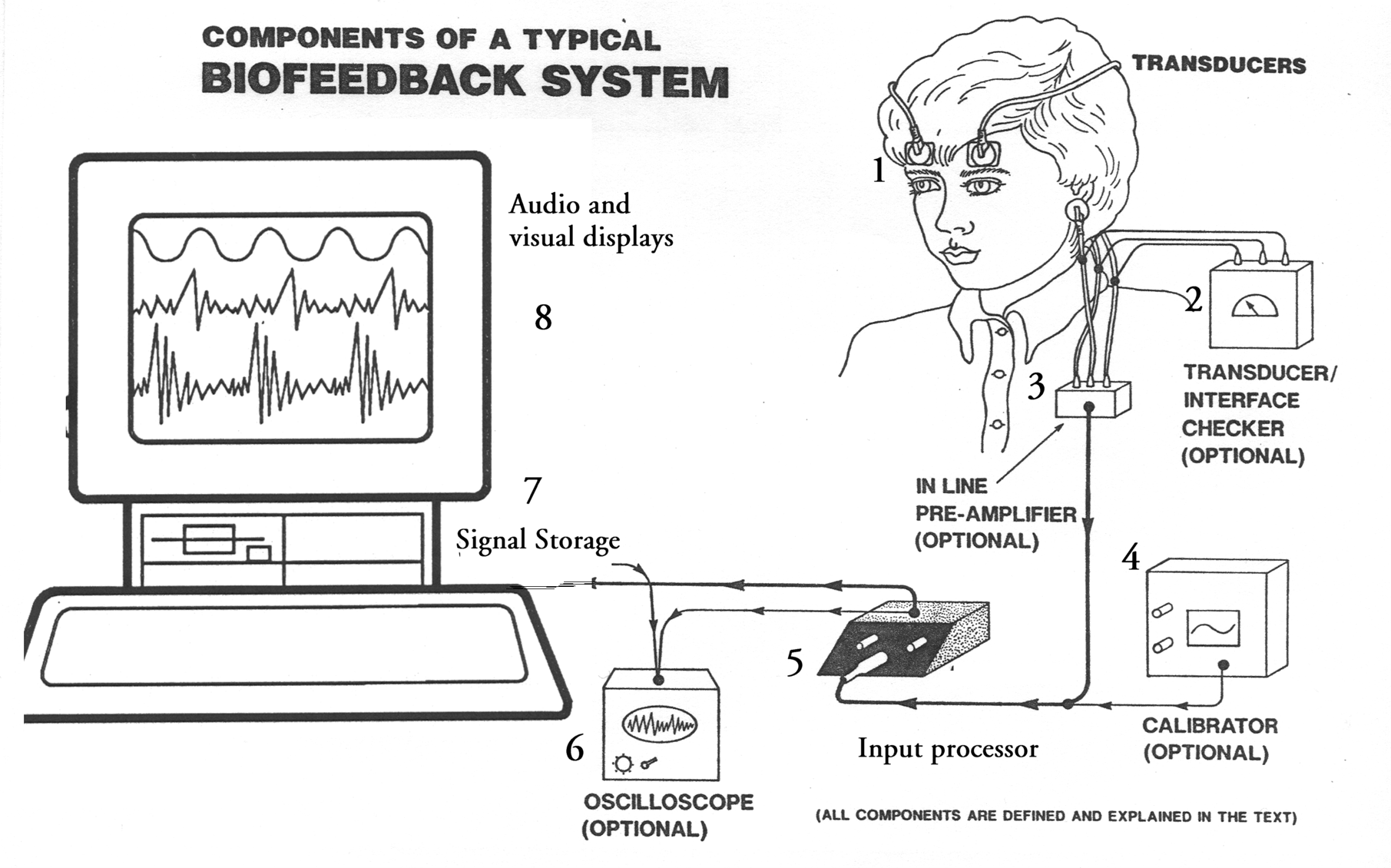
Modern biofeedback devices range from tiny ambulatory recorders to larger units meant to be used with personal computers. Virtually all of them are highly sophisticated, microprocessor based systems which can provide unparalleled quality and flexibility in signal recording and display. Nearly all of the controls are accessed through the computer’s software.
The essential components of a typical biofeedback device are illustrated in Figure 2. It shows a physiological signal being picked up by sensors adhering to the skin over the forehead and ear. The signals emanating from the skin are ionic rather than electrical in nature so have to be transduced into an electrical signal capable of being used by a typical psychophysiologic recorder (number 1 on Figure 2). The sensors have been carefully positioned so they can record from the muscle(s) of interest and applied so the signals can actually get off of the skin to the wires leading out of the sensors. The signals are amplified and adjusted to produce a display (8) which clients can use to learn to recognize levels at which parameters are functioning as well as their responses to various conditions. Clients use this knowledge to learn to control the parameters by using the display to inform them that their responses are correct.
Supporting references
Sherman R: Case reports of treatment of phantom limb and stump pain with a combination of electromyographic biofeedback and verbal relaxation techniques. Biofeedback and Self‑regulation 1(3): 353, 1976.
Sherman R, Gall N, Gormly J: Treatment of phantom limb pain with muscular relaxation training to disrupt the pain‑anxiety‑tension cycle. Pain 6: 47 ‑ 55, 1979.
Sherman R: Special review: Published treatments of phantom limb pain. Am. J. Physical Med. 59(5): 232 ‑ 244, 1980.
Sherman R, Sherman C, Gall N: A survey of current phantom limb pain treatment in the United States. Pain 8: 85 ‑ 99, 1980.
Sherman R: Direct evidence of a link between burning phantom limb pain and stump blood circulation. Orthopedics 7:1319 ‑1320, 1984.
Sherman R, Bruno G: Concurrent variation of burning phantom limb and stump pain with near surface blood flow in the stump. Orthopedics, 10: 1395‑1402, 1987.
Sherman R, Griffin V, Evans C, Grana A: Temporal relationships between changes in phantom limb pain intensity and changes in surface electromyogram of the residual limb. Int. J. of Psychophysiology 13: 71 ‑ 77, 1992.